Chairside 21
The Challenge of Saving or Extracting a Second Premolar (A Prosthodontic Case Report)
The patient came in asking whether tooth #5 could be saved. After completely removing the decay and the old restorations, only the buccal wall of the tooth remained.
Root length was favorable. Keeping the tooth would have required crown-lengthening surgery (CL) — about 3 to 4 mm of bone removal. Even after surgery, the tooth's prognosis would remain Fair, and the crown-to-root ratio would still be acceptable. But the real challenge was elsewhere: the adjacent tooth.
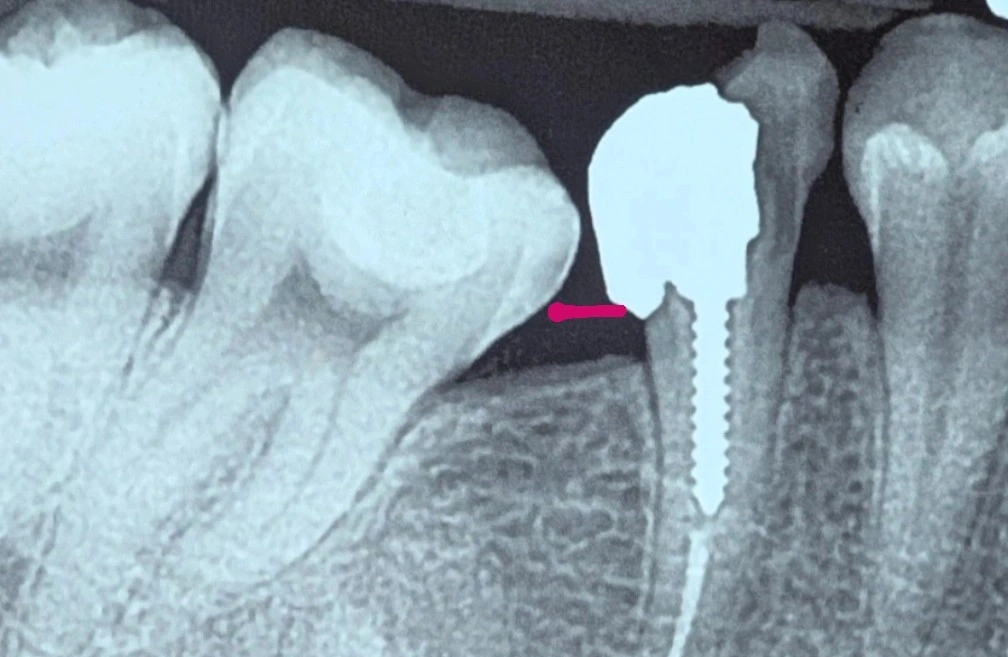
On the radiograph, the adjacent tooth (#7) shows a severe mesial tilt. Right now, the gingival level — marked with a red line — already limits food impaction because of the coronal attachment on tooth #7.
If CL surgery were performed and the bone and gingival level were lowered, the steep tilt of tooth #7 would change the local anatomy enough to create severe, progressively worsening food impaction. That would both cause the patient significant discomfort and raise the risk of caries on tooth #7 and chronic periodontal problems in the area. Saving one tooth would have put the adjacent tooth's health and the patient's comfort at risk.
Taking all of this into account, the more logical decision was to extract tooth #5 conservatively, preserving the bone for future implant treatment and preventing this chain of problems for the patient and the adjacent teeth.
The sequence toward this decision was as follows:
- Evaluating tooth #5 after complete removal of decay and old restorations; only the buccal wall remained.
- Considering the option to keep the tooth: root length was adequate, but it required extensive CL (3-4 mm of bone removal) and a final Fair prognosis.
- Identifying the real constraint: the severe mesial tilt of tooth #7, which would turn a lowered gingival/bone level into progressive food impaction.
- Deciding on conservative extraction of tooth #5 to preserve bone for implant treatment and prevent harm to the adjacent tooth.
️Sometimes the decision to keep a tooth has to be weighed against the health of the adjacent tooth, not just the prognosis of the tooth itself.
️A surgery that looks radiographically justifiable is no longer the right option once the adjacent tooth's anatomy won't allow it.
The content of this page is intended for the educational use of dentists and dental students.