Insight 47 — Key Points in Managing an Implant with an Unfavorable Angle
Published:
Last reviewed:
فارسی
Clinical Explanation
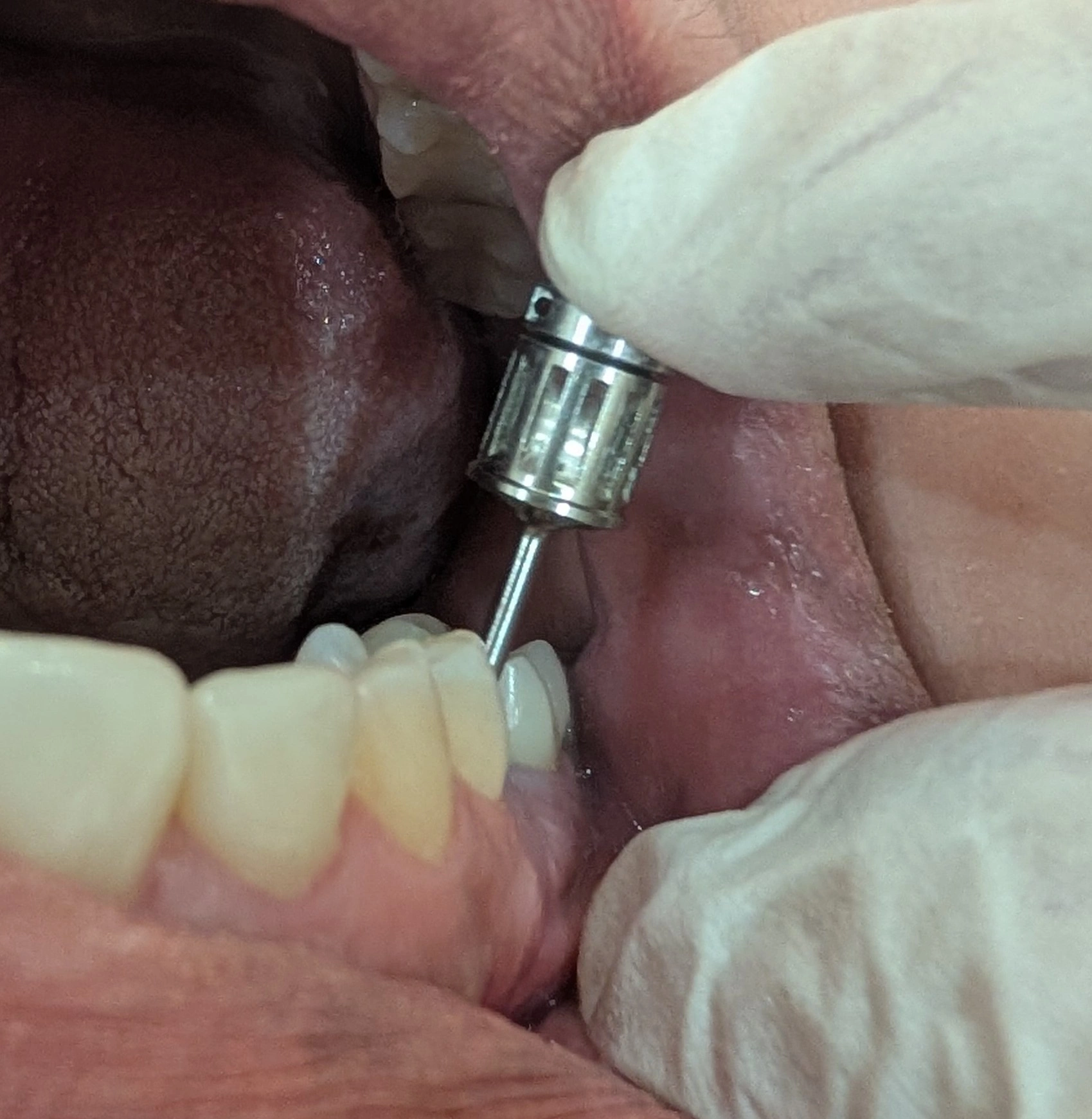
A posterior implant crown on a fixture tilted unfavorably in the buccolingual direction; why the angle is not merely an abutment problem, why here we should go for a retrievable crown rather than permanent cementation, and why in group-function occlusion we gently take the crown out of lateral contacts without disturbing the buccal cusp form
- When an implant's angle is unfavorable, the common assumption is that the matter is simple: you place a suitable abutment (for example, an angled abutment), correct the path, and that's it. As if the implant's angle is merely a path problem with no complication behind it. This assumption is wrong. The fixture's angle shows itself in later complications, and that is exactly why you must be careful when choosing the crown and the occlusal design.
- And the point is that not every angle is the same. What threatens the abutment screw is not merely being angled—it is the direction of that angle; and worst of all is the buccolingual angle.
- This implant was tilted unfavorably in the buccolingual direction, and that very direction determines everything. According to studies, the buccolingual angle is the worst for screw loosening. The reason is probably this: if the angle is mesiodistal, the lateral force vectors are largely restrained and corrected by the proximal contacts of the adjacent teeth; but in the buccolingual direction there is no such contact to take the force, so the load sits directly and non-axially on the abutment–screw assembly, and that is what loosens the screw. So when the angle is in this direction, we are effectively dealing with screw loosening. The first decision is clear: the crown must be retrievable, so that if the screw loosens you can get to it and retighten it without destroying the crown.
- The subtle point is this: the same buccolingual angle that raises the risk of loosening also throws the screw-access location onto the buccal. The screwmentable (screw-cement) approach was built exactly for this retrievability (you cement the crown onto a custom abutment and screw it down at the end), but its condition is that the screw-access hole comes out on the occlusal. When that access falls on the buccal, you effectively lose the conventional screwmentable option. If you can use an angulated screw channel to bring the access back to the occlusal, do exactly that; that is the best case, because retrievability stays in place and the access sits in its right spot. If even that isn't possible, it is better not to go for permanent cementation; permanent cement on an implant whose screw may loosen at any moment does not solve the problem, it only hides it.
- The second point goes back to the patient's occlusion, which was group function. In group function, during lateral movements several posterior teeth on the working side take up the guidance together, meaning the horizontal force reaches this crown as well. Now, even if the literature does not definitively confirm this vector on this particular tooth, on an implant that already carries non-axial load because of the angle, my preference is to reduce that very force. So in lateral movements I took the crown very subtly out of contact, in a way that the appearance—and especially the buccal cusp form—is not disturbed at all. The logic is the same implant-protected occlusion: as far as possible remove the guidance and horizontal load from the implant, without ruining its visual form.
-
Key takeaway:
Do not see an unfavorable fixture angle as merely an abutment problem; that same angle later shows itself in complications. More importantly, what threatens the screw is the direction of the angle, not being angled itself, and according to studies the buccolingual angle is the worst; probably because, unlike the mesiodistal direction, the contact of the adjacent teeth does not restrain the lateral force in this direction and the load falls directly on the screw. So on a fixture angled buccolingually, build the crown retrievable; if that same angle throws screw access onto the buccal, first try with an angulated screw channel to bring it back to the occlusal, and if that fails do not go for permanent cementation. At the same time, in group function reduce the horizontal load by gently taking the crown out of lateral contacts, so that the buccal cusp form and the tooth's appearance stay in place. In short, on an angled fixture prevent both screw loosening and horizontal overload, without losing esthetics.
The content of this page is intended for the educational use of dentists and dental students.