The patient had presented with a chief complaint in another area.
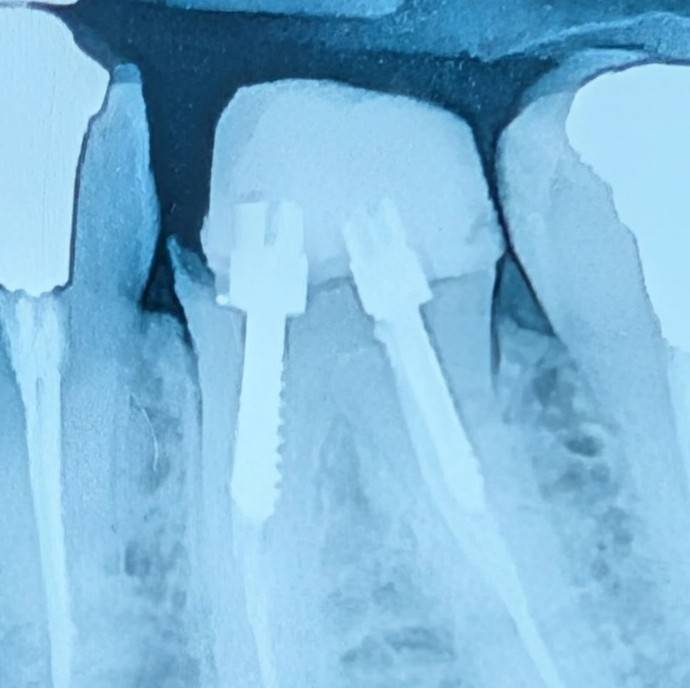
On examination, the lower left first molar (tooth 6) drew attention.
A poor-quality composite build-up restoration without a proper bond was seen,
accompanied by recurrent caries and leakage.
A considerable part of the coronal structure had been lost, and there was practically no ferrule.
Given the remaining condition of the tooth, if this tooth is to be preserved for a crown,
it would first require root canal re-treatment.
After that, to create an adequate ferrule, crown lengthening surgery would have to be performed.
But in this tooth there is an important limitation:
Given the position of the caries, the extent of structure loss, and the location of the bone and the furcation,
crown lengthening would likely come close to furcation involvement.
In such conditions, even if the treatments are carried out,
consequences such as food impaction and periodontal problems are to be expected.
Therefore, the treatment path to preserve the tooth is both costly
and accompanied by a guarded prognosis.
For this reason, the option of extracting the tooth and replacing it with an implant
was raised with the patient as the more logical treatment.
At this very point, an unexpected detail came up:
the patient said this tooth had already been prepared by another dentist
and that its crown was to be delivered soon.
This is the moment when, chairside, the main question takes shape:
when a tooth practically lacks a ferrule,
can a crown alone be expected to provide an acceptable prognosis?
And not even an ideal crown — but a crown that is to be placed over residual caries.
In such conditions, if the treatment fails,
the absence of a ferrule is probably one of the first factors
that will be raised in analyzing the cause of failure,
and the fault lies with the clinician
who undertook prosthetic treatment without a ferrule.
The content of this page is intended for the educational use of dentists and dental students.